
Functional Neurological Disorder, the Brainstem, and the Upper Cervical Spine
A systems-based root cause framework for clinicians, healthcare professionals, and deeply curious non clinicians who want a clearer way to think, assess, and collaborate.

Functional Neurological Disorder, the Brainstem, and the Upper Cervical Spine
A systems-based root cause framework for clinicians, healthcare professionals, and deeply curious non clinicians who want a clearer way to think, assess, and collaborate when “normal imaging” is not the end of the story.
If you were trained to think that “neurology equals lesions,” Functional Neurological Disorder (FND) can feel like a category error.
Patients show up with tremor, weakness, gait collapse, speech changes, sensory symptoms, seizure-like episodes, dizziness, brain fog, and autonomic complaints, and yet imaging can look unremarkable. Too often, the system responds with either dismissal (“it’s anxiety”), or a dead end (“we can’t find anything”). Neither is accurate.
FND is a diagnosis with positive clinical features, meaning there are exam findings and patterns that allow a clinician to rule it in, not a label we slap on after we run out of tests.
It’s also common. In large reviews, FND is described as one of the most frequent reasons for new outpatient neurology consultations, with some estimates around 1 in 6 referrals.
So why is it still so misunderstood?
Because FND lives in the space where brain networks, threat physiology, learning, attention, and context intersect. The “hardware” can be intact while the “software” is dysregulated. That does not make the symptoms less real, it makes the mechanism different.
Here’s the short version of what I shared recently on Instagram, the long version is this article:
“FND is not fake, and it’s not just anxiety. It’s a nervous system functioning problem, and stress, illness, or injury can lock the brain into an error loop. The brainstem and upper cervical inputs are often ignored, and in some complex cases they are the missing perpetuating factor. FND is nuanced, multifaceted, and needs multidisciplinary care.”
I’m Dr. Sina Yeganeh, D.C. Chiropractor, co founder of Movability, and a global complex case consultant. I work with clinicians and healthcare professionals around the world on complex chronic pain and mixed neurophysiologic presentations. This article is education, not personal medical advice.
The symptom pattern that confuses everyone
The pattern I want you to recognize is not “one symptom.” It’s a cluster:
Neurologic symptoms that can look dramatic, yet fluctuate
Symptoms that worsen under stress, overload, pain, poor sleep, hormonal shifts, illness, or after injury
Autonomic instability layered in (lightheadedness, palpitations, GI issues, temperature dysregulation)
Often comorbid migraine, chronic pain, fatigue, IBS, and dizziness, sometimes alongside a clear structural diagnosis too
And yes, many patients report stress as a trigger. But here is the nuance: in the best available synthesis, childhood adversity and recent stressors are risk factors with odds ratios often around 3 to 4, and yet over 50% of patients do not report those events in published studies.
So the simplistic story (“it’s all trauma”) fails, even when trauma is clinically relevant.
Who gets FND more, and why that matters clinically
Across large studies, women are disproportionately affected, commonly quoted in the 60 to 80% range, with a narrower gap in early and late life.
That is not a punchline. It is a clinical signal. It forces us to take seriously how biology, social context, threat exposure, healthcare bias, and patterns of care interact. It also forces us to avoid reducing women to “stress cases.”
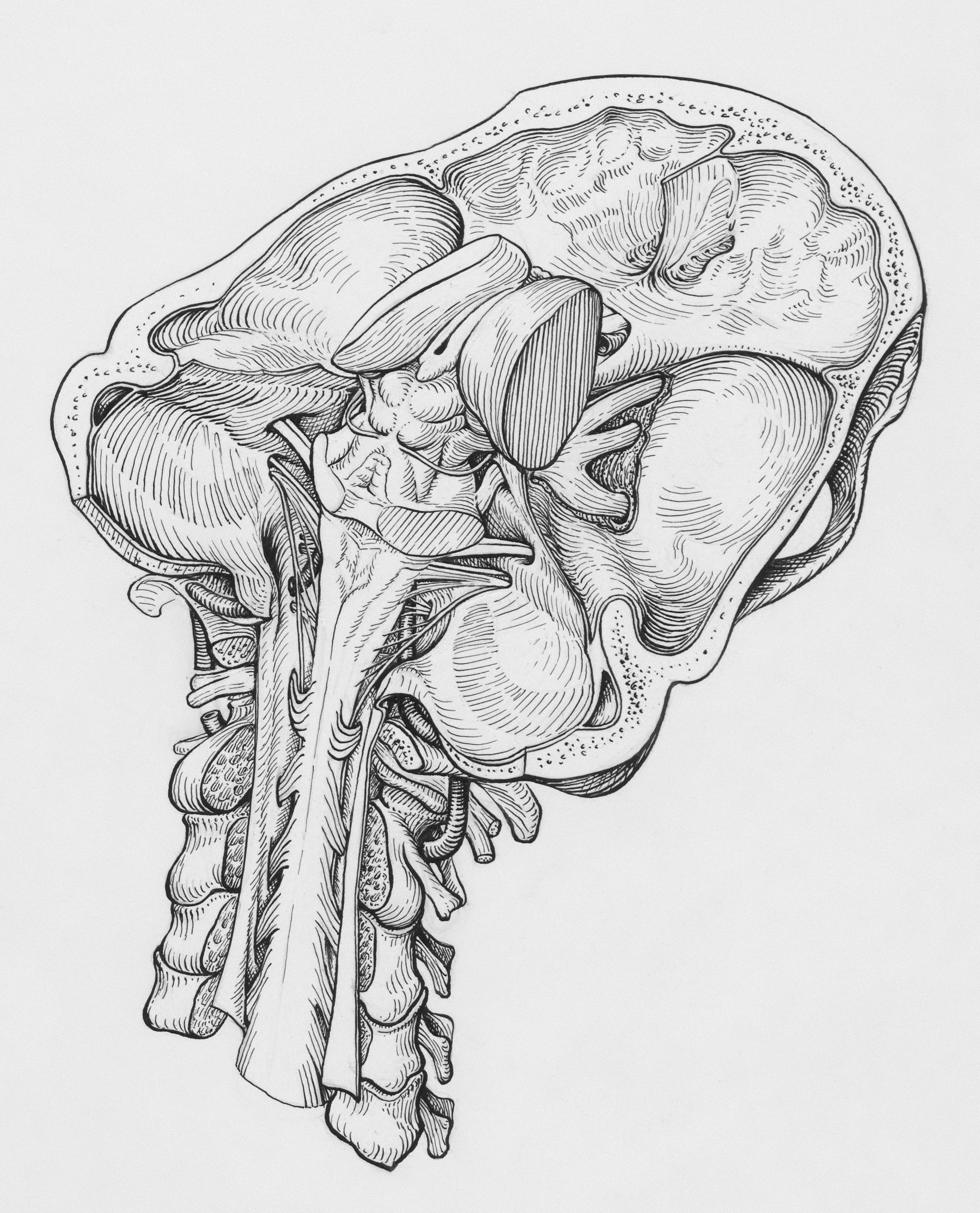
The brainstem and upper cervical piece that gets skipped
Most public education on FND focuses on cortical networks (attention, agency, prediction). That is useful, but incomplete for many complex cases.
The brainstem is where threat physiology becomes body physiology: autonomics, breathing rhythm, vestibular processing, arousal regulation. The upper cervical spine is a high density sensory input zone feeding that brainstem, integrating head position and movement with vestibular and visual signals.
That is why, in the real world, the patient whose “FND” looks like dizziness, gait instability, visual motion sensitivity, episodic weakness, and autonomic surges may not improve if we only chase the symptom in isolation.
Neck and brainstem inputs do not “disprove” FND. Sometimes they perpetuate it, sometimes they mimic it, sometimes they coexist, and sometimes they are the part nobody assessed carefully.
Why chasing symptoms fails
Conventional approaches often fall short when they over commit to one lens:
purely structural (“show me the lesion”)
purely psychological (“it’s stress”)
purely exercise based (“generic rehab will fix it”)
purely medication based (“we’ll sedate the nervous system”)
FND is a network disorder with layered drivers, and the most durable progress tends to come from a multidisciplinary plan that addresses motor retraining, autonomics, threat physiology, sleep, pain, vestibular and visual integration, and psychosocial context, without making any one domain “the whole story.”
