
When Jaw Clenching Creates “Sinus Pressure,” a Red Hot Cheek, and Facial Nerve Symptoms
A Root Cause Breakdown for clinicians and curious patients who want to understand TMJ, trigeminal nerve irritation, red cheeks, and sinus pressure can be one connected pattern.

When Jaw Clenching Creates “Sinus Pressure,” a Red Hot Cheek, and Facial Nerve Symptoms
A Root Cause Breakdown for clinicians and curious patients who want to understand how TMJ dysfunction, trigeminal nerve irritation, facial flushing, and “mystery sinus pressure” can all be part of the same system.
The Face Is Often Telling a Bigger Story
One of the biggest mistakes we make with complex facial symptoms is assuming the location of the symptom tells us the location of the problem.
A patient points beside the nostril and says, “I feel pressure here.”
Another says, “One cheek gets red and hot.”
Another says, “It feels like sinus pressure, but my scans are normal.”
Another says, “My teeth ache, my ear feels full, my eye feels heavy, and my jaw is always tight.”
Most of the time, those symptoms get separated.
The cheek is treated like a skin problem.
The sinus pressure is treated like a sinus problem.
The tooth pain is treated like a dental problem.
The ear fullness is treated like an ear problem.
The headache is treated like a headache problem.
The jaw tension is treated like a TMJ problem.
But in complex cases, the body is rarely that compartmentalized.
A red cheek, facial pressure, nostril pressure, tooth sensitivity, eye heaviness, ear fullness, headaches, and jaw clenching can all be different expressions of one deeper issue: an overloaded trigeminal nerve system.
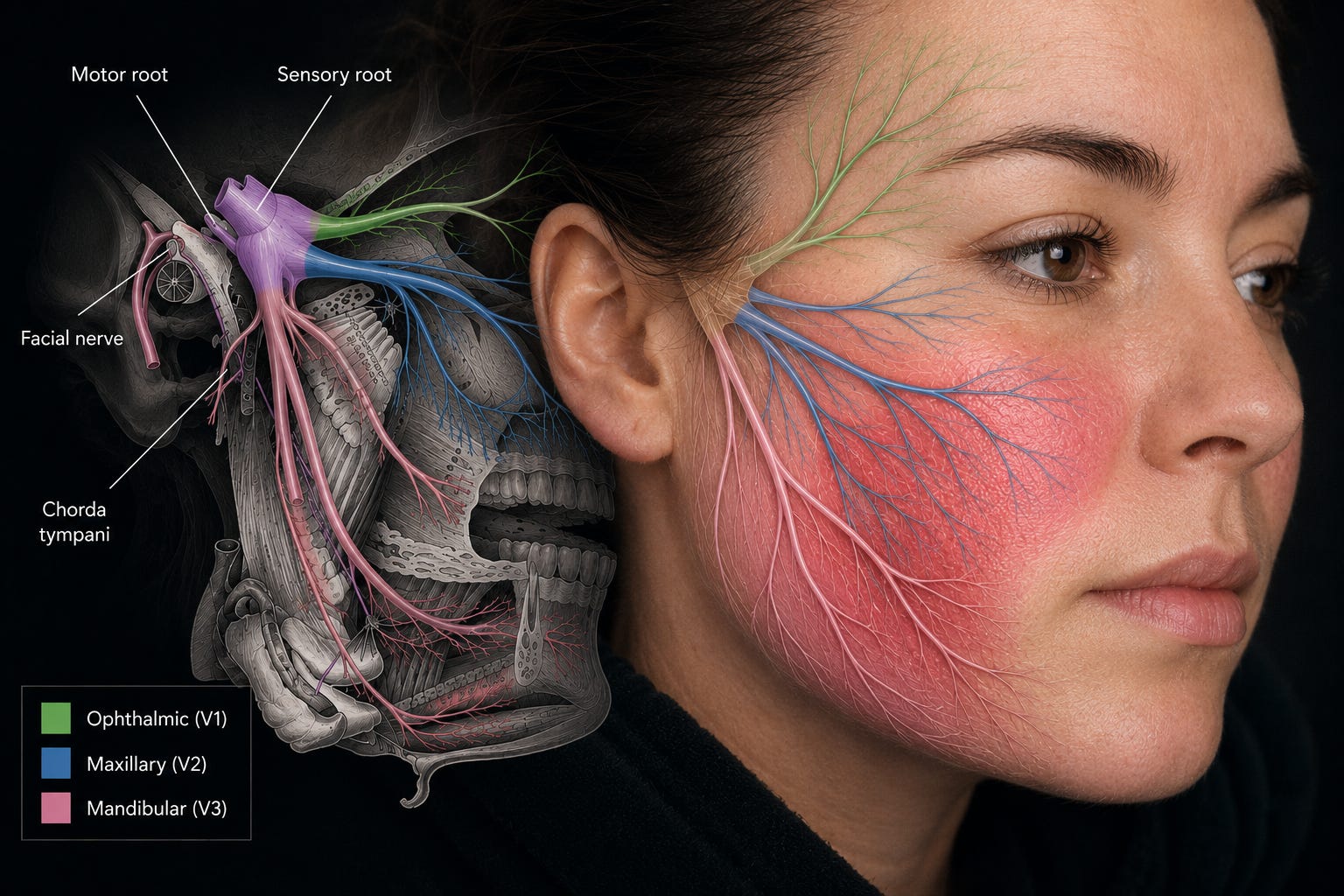
The trigeminal nerve is cranial nerve five. It is the major sensory nerve of the face, and it also provides motor control to the muscles of mastication, the muscles we use to chew. Its maxillary division, called V2, supplies the middle part of the face, including the cheek, side of the nose, upper lip, upper teeth, and maxillary sinus region. The infraorbital nerve, a branch of V2, supplies sensation to the lower eyelid, side of the nose, upper lip, and parts of the upper teeth. That anatomy matters because it explains why someone can feel “sinus pressure” beside the nostril without the sinus being the primary driver.
This is where jaw clenching becomes important.
When someone clenches, they are not just tightening the visible masseter muscle on the side of the jaw. They are loading the temporalis, medial pterygoid, lateral pterygoid, TMJ, teeth, periodontal ligaments, cervical spine, and the sensory pathways that report all of that information back to the brain.
Over time, that input can irritate, compress, or sensitize branches of the trigeminal system. In some patients, especially those evaluated by a TMJ specialist or orofacial pain provider, there may be a documented peripheral irritation or entrapment pattern. In others, the driver may be less about one nerve being physically compressed and more about the entire trigeminal system becoming too reactive.
Both matter.
The clinical mistake is thinking, “If the cheek is red, it must be skin.” Or, “If the pressure is near the nostril, it must be sinus.” Or, “If the tooth hurts, it must be dental.” Sometimes those are true. But not always.
A red, hot cheek can be part of a neurovascular response. When trigeminal pathways are irritated, inflammatory neuropeptides such as CGRP and Substance P can be involved in vasodilation, altered blood flow, and neurogenic inflammation. This same general biology is central to migraine physiology and helps explain why facial symptoms can include warmth, flushing, burning, pressure, and a sensation of swelling even when the problem is not simply local tissue swelling.
This is also why some headache and facial pain disorders come with autonomic symptoms: tearing, red eye, nasal congestion, facial sweating, and one-sided cranial symptoms. The International Classification of Headache Disorders describes trigeminal autonomic cephalalgias as conditions involving unilateral head pain with cranial autonomic features on the same side. That does not mean every red cheek is a headache disorder. It means the trigeminal-autonomic connection is real, and clinicians need to know how to recognize when the face is expressing a deeper nervous system pattern.
This matters because patients with these patterns often feel dismissed.
They have seen ENT.
They have seen dental.
They have seen dermatology.
They have had imaging.
They have been told, “Everything looks normal.”
And sometimes everything does look normal, because the issue is not always a visible lesion. It may be a system under load.
Of course, we do not skip red flags. A hot red cheek can be infection, cellulitis, dental abscess, allergic reaction, shingles, inflammatory disease, vascular pathology, or something else that needs medical attention. Progressive numbness, facial weakness, fever, severe sudden headache, vision changes, unexplained swelling, immune suppression, cancer history, or rapidly worsening symptoms should never be minimized.
But once the dangerous causes have been ruled out, we still need a better question than, “Why is this one spot symptomatic?”
The better question is: what system is being irritated, and why is that system staying irritated?
If you know someone who keeps being told their sinus, tooth, skin, ear, and jaw symptoms are separate problems, this is the kind of pattern worth sharing.
In the members-only section, we are going to map the full systems picture behind this pattern: how the trigeminal nerve, TMJ, pterygoids, infraorbital nerve, autonomic nervous system, migraine biology, cervical spine, airway, sleep, and stress physiology can converge into one facial symptom cluster. We will walk through the anatomy, biomechanics, and physiology in plain language, break down the symptom clusters and exam findings that matter, show the sequencing logic I use to decide what to rule in first and what to rule out early, identify where clinicians get misled, and finish with a short case vignette showing the pivot point where the plan changes.
Paid members get every weekly Root Cause Breakdown, the full archive, and a voice in what we cover next.
