When “Sinusitis” Is Not A Sinus Problem: Why persistent sinus pressure sometimes starts in the neck veins, not the nose
For clinicians, health professionals, and curious readers who suspect there is more to “chronic sinusitis” than blocked holes and bad allergies.

When “Sinusitis” Is Not A Sinus Problem
Why persistent sinus pressure sometimes starts in the neck veins, not the nose
For clinicians, health professionals, and curious readers who suspect there is more to “chronic sinusitis” than blocked holes and bad allergies.
Most people are told a simple story about chronic sinus symptoms.
Sinuses get blocked. Mucus builds up. Pressure equals infection. Treat the sinuses. End of story.
Except there is a large group of patients who never fit that story.
These are the people who have lived on and off antibiotics, nasal steroids, sinus rinses, antihistamines, even sinus surgery. Their scans may be unimpressive or “post surgical but clear.” Yet they still wake up with pressure behind the eyes, heaviness in the cheeks, a tight band across the forehead, or a strange mix of stuffy and dry that never really settles.
In my clinic, a surprising number of these patients do not primarily have a sinus problem. They have a drainage problem. More specifically, an outflow problem in the veins of the head and neck.
Here is the pattern I see again and again.
The patient reports “sinus” pressure that is:
Strongly position dependent. Worse with long screen time, looking down, certain lifts, or a particular sleep position.
Reproducible from the neck. When I examine their upper cervical spine, first rib, jaw, and the soft tissues around the internal jugular vein, I can often reproduce their “sinus” pain almost exactly.
Weirdly resistant to sinus focused care, yet surprisingly responsive when we change neck mechanics, rib motion, and breathing.
On imaging, their sinuses may look “fine enough.” What rarely gets checked is how the nose, sinuses, and deep facial structures drain into the venous system, and what happens to that outflow when you put a vulnerable neck into a provocative position.
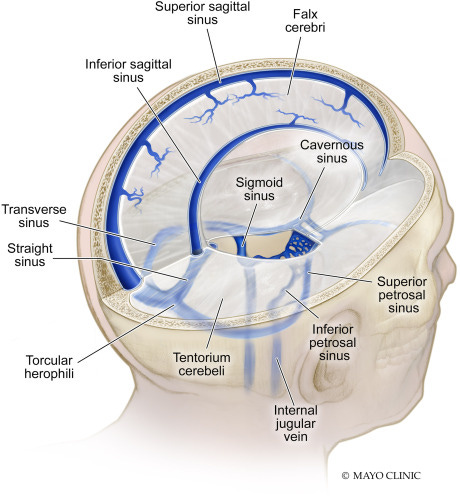
The idea that chronic sinus pressure can be driven by venous outflow is not news in basic anatomy texts. The nasal cavity, gums, teeth, and paranasal sinuses drain into a network of veins that ultimately converge on the internal jugulars and the venous plexus that runs along the spine. If you pinch or collapse those exit ramps, blood does not stop. It detours. Pressure redistributes. Structures with rich venous cushions, like the turbinates and sinus mucosa, swell. Patients feel this as pressure, fullness, or congestion, even when there is no active infection and the ostia are technically open.
Clinically, this shows up most clearly in three groups:
People with long standing “sinusitis” that never quite matches their scans.
Patients with upper cervical issues, whiplash, hypermobility, or scoliosis who also report sinus, ear, dental, or gum pressure that behaves strangely with posture.
Patients with unexplained ear fullness, facial pressure, or “migraine” symptoms that are consistently linked to neck position, but have normal ENT and neuro workups.
These patients fall into a gap between specialties. ENT quite reasonably focuses on the air cavities, mucosa, and local inflammation. Neurology may focus on migraine patterns and central sensitization. Musculoskeletal providers look at joints and muscles. Vascular structures are often mentioned briefly in anatomy class, then largely ignored.
When you treat only what you can see on sinus CT, or you only chase pain where it is felt, you can miss the plumbing problem sitting a few centimeters lower in the neck. You also miss the way cervical mechanics, breathing, rib cage behavior, autonomic tone, and even desk setup can converge on that same venous system.
This article is my attempt to lay out a more complete map.
We will walk through the venous anatomy in plain language, translate it into symptom patterns, and look at why conventional care so often fails this subset of “sinus” patients. Then we will zoom out to a systems view so you can see how jaw, neck, ribs, breathing, and autonomics interact with venous outflow.
If you work with complex pain or stubborn ENT type complaints, my hope is that you will come away with a clearer pattern in your mind and a more structured way to investigate it. If you are a non clinician who has lived this story, I want you to see that your symptoms make anatomic sense, even if no one has ever explained it to you.